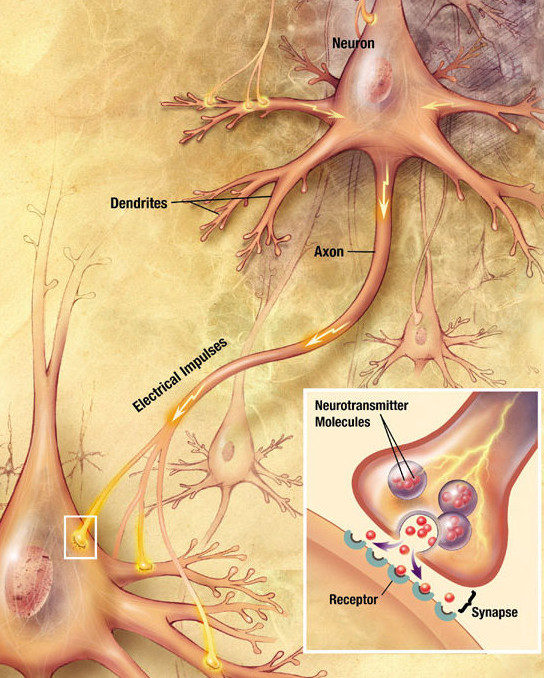
Medication commonly used in the treatment of seasonal affective disorder (SAD) or winter blues, belong to different groups of antidepressants. They are all designed to target specific receptors on different parts of nerve cells in order to change the concentration of certain neurotransmitters in the brain. Neurotransmitters are substances which are produced by nerve cells, and they allow the communication between nerve cells, so therefore, the optimization of their concentration is very important for the normal functioning of the nervous system.
There are several groups of antidepressants, but those from second generation are proven to be the most beneficial for patients with SAD. They include selective serotonin reuptake inhibitors (SSRIs), serotonin and norepinephrine reuptake inhibitors (SNRIs), and other medication with more complex mechanisms of action.
Selective Serotonin Reuptake Inhibitors (SSRIs)
Selective Serotonin Reuptake Inhibitors are most commonly used drugs in treatment of winter blues, and they are available worldwide in many forms. Some of them are: paroxetine, fluoxetine, sertraline, etc. They are also the very first medications developed to target specific receptors in the brain. SSRIs are designed to block the degradation of serotonin, and they act as a part of a very complex mechanism which involves several phases. The end result of that process is the increase of serotonin levels in neural tissue which is shown to significantly improve the symptoms of SAD.
The first effects of the treatment with SSRIs appear after 1-3 weeks of treatment, but the full effect is not developed before 6-8 weeks. These antidepressants tend to have sedative effect at first, but as the antidepressant effect becomes stronger during several weeks of treatment, the sedation lowers.
Serotonin and Norepinephrine Reuptake Inhibitors (SNRIs)
Another class of antidepressants used in the treatment of SAD includes serotonin and norepinephrine reuptake inhibitors (SNRIs). These drugs are blocking the degradation of two neurotransmitters – serotonin and norepinephrine, thus increasing their concentration in neural tissue. Besides their wide use for beating the winter blues and other depressive disorders, they are also used for relieving symptoms of chronic neuropathic pain and for obsessive – compulsive disorders. Some of these medications are venlafaxine, desvenlafaxine, duloxetine, etc. Because of their dual mechanism of action, these drugs affect a number of different neurotransmitters and have a stronger mood-changing effect than SSRIs. However, they are considered second line therapy because of broader range of side effects than SSRIs, and are used only if SSRIs are ineffective.
Other Drugs Involved in SAD Treatment
Lots of drugs with different mechanisms of action were developed in addition to standard therapy. Bupropion increases the concentration of norepinephrine and dopamine (another very important neurotransmitter) in neural tissue. Increase in dopamine levels contributes to better mood, improves psychomotor functions, and beats sleepiness and craving. Desipramine belongs to tricyclic antidepressants (TCA) and it is predominantly a norepinephrine reuptake inhibitor. They are old generation antidepressants which have proven to be beneficial for the treatment of SAD, but because of their numerous side effects, they are now replaced with new generation drugs which were mentioned before, that have significantly less side effects.
When to take the drugs?
Any of the SSRIs will usually be recommended for use before the initial symptoms of SAD begin. That way, the negative feelings and lethargy that regularly occurs from November through March each year can significantly be eliminated or reduced. Antidepressant therapy works in concert with a healthy diet, counseling, and phototherapy (using a light box), to beat the winter blues. Check with your physician as to the course of treatment that is best for you.
Did you enjoy this post? Sign up for our newsletter to be informed about new articles!
[hb_button button_title=”Sign me up for the newsletter!” target=”_blank” button_size=”large” button_color=”#f79124″ button_link=”http://www.beatthewinterblues.info/newsletter-signup/”]
References
Kurlansik, S.L., Ibay, A.D. (2012). Seasonal affective disorder. Am Fam Physician. 86(11):1037-41.
Gupta, A., Sharma, P.K., Garg, V.K., Singh, A.K., Mondal, S.C. (2013). Role of serotonin in seasonal affective disorder. Eur Rev Med Pharmacol Sci. 17(1):49-55.
Spevack, L. (2011). Beating the winter blues: helpful hints for the season and beyond. Diabetes Self Manag. 28(6):6-8, 10.
Molnar, E., Gonda, X., Rihmer, Z., Bagdy, G. (2010). Etiopathology and therapy of seasonal affective disorder. Neuropsychopharmacol Hung. 12(4):483-94.
Trackbacks/Pingbacks